


Who is it that benefits from health records rules and medical records projects?
Because it certainly isn’t the patients...

Over the last week I and, to the best of my knowledge at least one other person investigating the issues surrounding the Lucy Letby criminal investigation and trial, have been directly or indirectly threatened - ostensibly by or on behalf of Cheshire Police. Yes, the same Cheshire Police who, if elected mayor, Nick Buckley MBE has vowed to sack for failing to detect and deter real crime and instead wasting public resources and time spouting woke rubbish.

It seems some umbrage has been taken to anyone publicly pointing out obvious facts like that the ‘experts’ (for example, Dr Dewi Evans) that they chose to front the prosecution side of the case are in fact not experts in neonatology, and hence their evidence is little more than ipse dixit (unsubstantiated opinion). They also don’t seem to like that people have pointed out that Dr Evans’ involvement was via his profit-making ‘expert witness consultancy’ company Dewi Evans Paediatric Consultancy Plc and that he, as defence counsel so correctly pointed out, came to Cheshire Police touting for business. That is to say, he was not approached as a known or accredited expert in neonatology. Rather he, by his own testimony under cross examination, drove to Cheshire after having already formed his own opinion that something nefarious was going on in the CoCH neonatology unit, and insinuated himself into the investigation. I realise that in 2023 too many people believe facts are not facts unless the government and mainstream media fact checkers deem them so, so I am withholding my next two articles on my own investigation of the justiciable facts for at least a few days - possibly until after the verdict is rendered.
Electronic Patient Records
Over the last several years significant amounts of money have been spent in the UK and every other western country on a variety of often disparate electronic medical records (EMR) or electronic health records (EHR) systems and solutions.
Collectively, we have been sold EMR/EHR (hereafter simply EHR) under a number of what I believe have been false pretences that often boil down to the misconception that ‘going digital’ in healthcare will bring convenience, improved outcomes and safety benefits. Yes, some claim that EHR will magically reduce clinician burnout, improve the work-life balance for clinicians, revolutionise your business or reduce healthcare costs - but most of these claims read more as mere puffery1. The key claims often centre on some or all of the following - that implementation of EHR will provide for:
accurate, complete and up-to-date information at point-of-care
faster access to patient information
coordinated and efficient care, especially where the patient is cared for between multiple providers
secure sharing of patient information with patients and other healthcare providers
more effective diagnosis of patients
a reduction in medical errors
safer care
more reliable and safer prescribing
legible, complete documentation
accurate and streamlined billing
If you critically appraise that list, all of the items distil down to increased convenience for patients or clinicians or improved outcomes and patient safety.
This brings us to the first question: After more than two decades in use, have the claimed benefits of EHR actually been realised?
First, let’s consider the simplest form of the main claim: that EHR increase accuracy. Several studies have investigated the accuracy of information in EHR and found errors in as many as 20% of all EHR, with 40% of those errors characterised as serious errors2. In a useability and safety test conducted with experienced emergency medicine clinicians and the two most common EHR systems used in hospitals, error rates of 35% were recorded for simple tasks like ordering an X-ray of a patient’s left arm, and error rates as high as 50% for tasks like entering a multi-dose medication prescription3. A 2018 Pew study found that as many as 1 in 5 patients may be mis-identified or not accurately linked to the correct EHR4 - something that was seen in the evidence from the recent Lucy Letby trial in the UK where an experienced neonatal nurse and Deputy Ward Manager entered clinical notes regarding a neonate that died in her unit, into another living neonate’s EHR5.
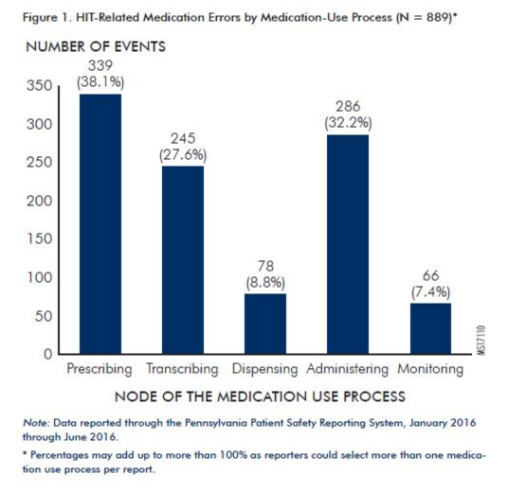
Next, let’s consider whether implementation of EHR brings more reliable and safer prescribing. Most hospitals and GP clinics use EHR systems that are promoted as being capable of identifying and alerting the clinician to prescribing errors - instances where the drug being prescribed is contraindicated for this patient due to a demographic predisposition, allergy, interaction with other drugs the patient is already taking, or for some other medical reason. A recent study resolved that these alert-capable GP and Hospital EHR systems still fail to identify more than 33% of drug-diagnosis contraindications (for example, when a person with hemochromatosis is incorrectly prescribed iron preparations or when a pregnant woman is prescribed a teratogenic drug such as Thalidomide or Isotretinoin) and fail to alert clinicians to almost 62% of drug-age contraindications (for example, when a child or teenager has a viral infection and is prescribed aspirin, which can cause Reye Syndrome)6. A study by the Pennsylvania Patient Safety Reporting System identified 889 health-IT related medication errors occurred in the State’s hospitals during the six month period from January to June 2016, and found that 70% of all health-IT related medication errors reached the patient7. They concluded health-IT related medication errors are massively underreported and that every day we are risking serious patient harm.
Finally, let’s consider whether EHR lead to more effective diagnosis of patients. It has been claimed that access to the EHR at the point-of-care provides the clinician with more information and hence increases diagnostic accuracy. However, such studies are confounded by use of integrated cross-provider simulated ‘perfect’ patient records that don’t reflect the variability in quality seen in real-world EHR, and while claiming EHR increased the quality of diagnostic decisions, actually report dramatically inconsistent results8.

A review published in January 2023 found we currently do not fully understand the significant risk and diagnostic errors EHR introduce into the diagnostic process. The authors identified that many common EHR use issues concern the low quality of and errors in patient data (63.6%), poor design of the EHR user interface primarily in the areas of data entry (36.3%) and workflow processes (18.1%), and overall in the clinician’s ability to perceive and process the additional information presented to them by EHR9.
While we are still being told that implementation of EHR would increase clinical efficiency, studies as far back as 2005 showed that when juxtaposed against the use of paper records and clinical forms, EHR were exceedingly inefficient and more than trebled the amount of time nurses and doctors spent on record keeping10. More recent studies have shown that clinicians spend more time reviewing, documenting and ordering within the EHR11; possibly as much as double the time spent talking with and treating the patient12. Computers have replaced patients as the largest beneficiary of time during the nurse or doctor’s working day.
Rather than suggesting EHR deliver the promised accuracy, reductions in medical errors and improved safety at the point-of-care, the results of many studies tend towards showing that EHR may actually be doing the exact opposite. Not only are they not bringing the claimed benefits expected from the significant expenditure spent in their implementation, but they may be increasing complexity, confusion and inaccuracy, causing treatment delays and negatively affecting patient care and outcomes. It might also be said that they draw significant funds away from other more deserving areas that could see us safely treating greater numbers of patients: like maintaining and expanding facilities, ensuring adequate staffing numbers, unbiased ongoing research, training and public health initiatives.
EHR in the UK Context
In the UK these projects range from the records systems used: (i) at point-of-care such as Liverpool Women’s Hospital’s (LWH) Digital Generations and King’s College Hospital’s (KCH) Apollo, which are both ongoing implementations of new EHR systems; to (ii) area-wide projects such as the East London Health and Care Partnership (ELHCP) which has spent tens of millions of pounds on expensive Cerner technologies to establish the East London Patient Record (eLPR) which, they admit, does little more than feed into the entirely different technology platform purchased to support the One London Care Record (OLCR).
In the case of point-of-care projects, each individual Trust, and sometimes even each facility within the same Trust, use entirely bespoke implementations of several different underlying vendor platforms. For example, LWH’s new implementation is using Meditech while KCH is using EPIC. However, one thing that is consistent to all implementations in the NHS - whether point-of-care, regional or national, all implementations have or are running into common IT project issues that are causing: (i) frustration for clinical staff; (ii) significant additional cost that is borne by the taxpayer; and (iii) potential impact to the provision, quality and safety of patient care.
LWH’s Meditech deployment has been plagued with ongoing issues not limited to the fact that clinical staff feel like the system has not been properly designed and tested prior to implementation. Rather than ensuring concurrency between old and new systems so that the impact on patient care could be minimised, Meditech’s implementation process has been to disable the old maternity patient records platform while data was migrated from old to new: leaving staff with no access to a key EHR resource and unable to admit patients to maternity wards, order certain tests and medications, or record vital observations. Staff resorted to resuming the use of paper-based documentation that had not been in use in the hospital for more than a decade. Meditech and the hospital IT Support team had staff on the maternity units ostensibly to help, except that when nurses and midwives approached those staff, their assistance was limited to “I can’t do it either” and “I don’t have access to fix that for you”. Meditech and Trust IT staff didn’t even bother to do the simple step of reviewing the staff lists for the two shifts where they would be bringing the Meditech solution online, in order to prioritise creation of those staff user accounts. Instead, members of staff were told during handover that the new system was operational - only for the staff members to find at the critical point where they were dealing with a labouring mother that they had what one midwife called “an existential crisis”. They were not defined in the LWH ‘universe’.


(Maybe LWH’s problem is that they are still trying to complete the 2014/15 electronic patient records project concurrent to the 2023 project that is presently underway – because this text from their website suggests both projects are running concurrently. Screenshot captured July 11, 2023)
KCH’s issues include that they are months overdue due to data transformation issues, and significantly over budget. This, on top of the fact that KCH’s partner hospital Guys and St Thomas’ had already suffered more than a week’s complete absence of EHR as a result of the Trust’s IT staff not understanding and adhering to some of the most basic design rules we tech people are taught for IT datacentre environment management and redundancy.

So who are EHR benefiting?
We have seen that patients and clinical staff are not receiving the promised benefits of EHR, so at this point we come back to the question posed in the title of this post. Who is it that is benefiting from adoption and implementation of EHR?
1. The companies that develop, patent or own the EHR software
For example, in 2021 Cerner’s annual turnover in the UK was slightly more than £100mil13; Meditech’s was £186.1mil; EPIC’s was just over £100mil; TPP Group’s (SystmOne) was almost £76mil14; and EMIS Group’s exceeded £168mil15. In total, and for just these five vendors, the wider NHS has been spending as much as £630mil annually on EHR implementations and support services.
2. Organisations that sell access to or information learned or aggregated from harvested patient records datasets such as NHS Digital, HDRUK, Ben Goldacre’s Nuffield research group who run openprescribing.net and opensafely.org
HDRUK turnover rose from £27.4mil in 2021 to £64.6Mil in 2022. Some of that turnover is paid in the form of grants and stipends to Ben Goldacre’s Bennett Institute for Applied Data Science at the Nuffield Department of Primary Care Health Science - who collectively from some two dozen funders16 are estimated to receive more than £50mil annually. It was estimated in 2019 that NHS Digital turnover from the sale of our health data exceeds £5bn annually (with costs of more than two thirds of that). Very little of the NHS Digital funding is returned to the NHS Trusts in question.
3. Research partners with whom different NHS Trusts form financial research and data contracts and allow to access patient records datasets - such as Google’s Deepmind and Babylon AI.
Babylon Health had a turnover in excess of £32mil in just the UK in 2021, with their income almost entirely derived from grants and non-refundable payments from the UK government and the NHS - essentially your tax dollar at work. Further, Babylon Healthcare Services who ran the Babylon Digital Health Clinic had additional turnover of more than £24mil during the same year for their digital medical clinic using their differential diagnostic digital doctor iphone ‘app’ that Hannah Fry once quipped ‘didn’t know it’s arse from it’s elbow’17 that has since been shuttered, leaving more than 100,000 NHS patients without a GP service. DeepMind Technologies had a turnover of more than £1.36Bil18 however, after it was revealed that NHS contracts unlawfully allowed DeepMind to appropriate more than 140,000 EHR from UCL’s London servers into their Google parent company’s California datacentres, the NHS have refused to disclose how much of DeepMind’s annual income is derived from the ongoing NHS health records-based AI projects.
Clearly these three groups are profiting from our EHR while we fail to receive any of the claimed benefits.
In conclusion
One final issue means that the excessive wastage of taxpayer funds will continue to happen unrestrained. That is the fact that in the UK each NHS trust is allowed to select, fund (with your tax money) and maintain their own bespoke implementation of whichever EHR platform they chose - and in many cases several different platforms within the same hospital. This significantly decreases the portability of staff skills because most of what they learn and become familiar with is only applicable to a single hospital, and means that if staff move between hospitals they must be retrained to use the EHR systems at each hospital.
The clear and obvious solution to this is a national EHR platform that all Trusts and Hospitals would be required to use. Given that many hospitals and GP practices are choosing to use cloud-based platforms for EHR now anyway (I am looking squarely at you Meddbase and SystmOne... and at least two very recent multi-million pound implementations I have seen of Cerner Millennium), the use of a single national cloud-based solution operated by the health ministry would seem consistent with their current decisions.
Where such a national EHR would bring improvements is by: (a) reducing costs because individual NHS Trusts and Hospitals would no longer be involved in contracts for the implementation and support of expensive multi-million pound commercial EHR platforms; (b) reducing the current lack of interoperability and clinical data sharing between healthcare providers across the entire UK; (c) improving diagnostic and treatment decisions and reducing the potential for errors by ensuring every clinical team member who cares for a patient has access to the same patient record; and (d) ensuring all clinical staff no matter which facility or site they find themselves working on, can be trained on and are using a single familiar platform.
The UK patient and taxpayer populations need to rise up and demand the promised benefits of all this EHR spending. And the most obvious and possibly singular way those benefits can ever be realised is when we stop having hundreds of bespoke EHR implementations...
And invest in a single national EHR solution.
(or return to paper-based clinical systems)

Your analysis is oh so close, but misses the primary point. I was one of the designers of the original NHS National Spine that was never implemented (Thanks, Richard Granger). The point of that design (the closest I have ever seen a government come to getting it right) was that health records need to be about PATIENTS and in the UK there should be only a record per patient, oriented toward that patient.
The conceit in your article is that having a single EMR will "fix" this. The problem with all of the systems you list is that NONE of them actually is modeled around an individual -- the are all modeled around encounters, beds, institutions, visits, GP Practices -- anything but a patient. So you could install one of these classic EMRs for everyone and things would hardly improve.
The solution is still an individual-centric overlay that UNDERSTANDS the data (not just moves it around) and that takes it from all sources and makes it, credibly, be about YOU -- for your sake and the sake of all your practitioners. The UK missed its best opportunity in the last 30 years to achieve that when the National Spine was neutered.
Now with the emergence of Cognitive-AI (NOT the LLMs and deep learning engines which are probabalistic/inferential and not qualified for patient care) the opportunity to build individual-centric (NOT venue centric) records for each patient will be come available again. If the UK (which, with the NHS, should have perhaps the easiest worldwide shot at doing this) is to go down a different pathway, moving to a knowledge-centric (not repository centric) individual records approach will provide many of the solutions you seek. The "Epic everywhere" approach does not do it because the information is never understood (none of the systems you list have the capability -- that is not their point) and therefore individual-centric outcomes are permanently elusive.
A mention to the EPR of the IT system: TRAK, implemented in NHS Lothian since 2010, and licensed until 2040!