
LL Part 16: Basic Math - Part 2
Here's why even basic math is hard

Following on from our previous post here.
Like anything else in life, there is more than one take on which numbers you should or should not use as evidence for your conclusions.

Several people pointed to three issues with the previous post:
That I had used a 2021 national average for the underweight and premature babies percentage (from the Nuffield Trust website);
That I had used the Epicure study percentage for 22-26 week gestation babies whilst the CoCH even in Level 2 LNU mode should only have been taking babies of 27 weeks gestation or above; and
That there was a typographical error on the report I sourced that said there were 600 births annually at CoCH. This number was actually the number of beds in the entire hospital and the report author (thankfuly not me this time) had transposed it into the wrong box. The annual number of births at CoCH has been between 2,104 and 2,295 during the last several years (avg: 2,157)
Issues 1 and 2 are entirely accepted. Issue 3, whilst not of my doing, is also accepted.
In order not to bore everyone with long and complicated “get this number from that report, add it to this other number, multiply that by the factor in this third table and voila”, I tried to draw on some already pre-packaged and easy to use numbers that others had already developed and, those making the valid criticisms above rightly point out, I have ended up with a more-than-rosey final result.
Prematurity
Prematurity comes in three flavours:
Extremely Preterm (<28 weeks gestation)
Very Premature (28 - 31 weeks gestation)
Moderate-to-Late Preterm (32 - <37 weeks gestation)
For the CoCH hospital neonatal unit we are primarily dealing with the last two (Very Premature and Moderate-to-Late Premature). However, several of the people who pointed to the issues above also led that the cut-off value of Extremely Premature meant that no baby born <28 weeks gestation could ever end up in the CoCH neonatal unit or have died there. That is also an incorrect assumption. We must also incorporate a percentage of Extremely Premature because invariably some of these babies will be born at the hospital and, if protocols are followed, they will be stabilised for a period before being transferred out to Arrow Park or Liverpool Women’s Hospital (LWH). We also know that CoCH doctors liked to stretch the definitions of those protocols as far as they could - the 800 gram baby I mentioned in the previous post is one such example. The midwives at LWH this evening confirmed for me one possible reason why.
It seems that there is some sort of “accounting thing” between hospitals whereby as patients get transferred between them for various reasons, money changes hands as well.
Let’s say I am a consultant at LWH and I have a woman on the induction ward ready to go, and I have a NICU incubator waiting for her baby in the neonatal unit just in case. Her ‘case’ - her baby in effect, is worth a particular value per day to our unit. However, if at the same time CoCH rings up and has a 790 gram baby that needs to come over to our NICU, our unit will get more money per day based on our accepting that high acuity transfer from CoCH and therefore it is in our financial interest for the consultant to delay our own patient in the induction ward, and accept the transfer instead. This apparently can be very frustrating for the midwives, as the consultants can make these decisions and upset what might already be a carefully balanced ‘apple cart’.
But it can bring in some much needed extra funds to the unit and the unit gets paid a higher amount for providing the same acuity level of care that they might otherwise have given to a neonate born in their own hospital.
Interestingly, consultants at CoCH can make the same decision in reverse. If transferring that baby is going to cost their unit an expensive high acuity per-day fee, finding a way to keep the baby on your own unit can ‘seem’ more fiscally responsible. Well, if nothing else it is cheaper to look after your own patient yourself so it keeps the costs down. Possibly (and I am by no means saying this actually happened - merely that it might explain why some very small and extremely premature babies still show in CoCH’s statistics), a baby might be given a 10ml bolus of fluids, some medicines, or a number in the computer gets rounded up… or perhaps the consultant makes an arbitrary suggestion that the baby be characterised as ‘stable’ and ‘doing well’…1
And the baby stays in the home unit.
Money is saved. Nobody is really hurt.
Well, maybe nobody in a white coat carrying a stethescope...
Getting back to the numbers
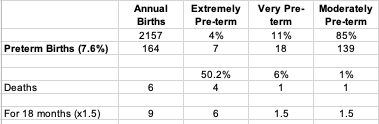
I went back to basics and pulled the ONS, MBRRACE, Nuffield and Tommy’s Data for 2015 and 2016 - and using all four sources found that for England and Wales the percentage of babies born:
Pre-term = 7.6% - of which:
extremely pre-term (<28 weeks gestation) = 4%
very pre-term (28 - 32 weeks gestation) = 11%
moderately pre-term (32 - <37 weeks gestation) = 85%
underweight (below 2.5kg) = 6.1% (
very underweight (below 1.5kg) = 4.9%
extremely underweight (under 1kg) = 4.3%
Unfortunately, the death data in the ONS report is provided on a ‘from birth’ basis:
early neonate = deaths <7 days
neonate = deaths under 28 days
postneonatal = deaths between 28 days and 1 year
Therefore, the ONS data doesn’t align sufficiently to allow us to directly calculate what percentage of each classification of pre-term died. What the ONS tend towards, is the giving of ‘rates per 1000’ (per1000) or ‘age standardised mortality rates’ (ASMR) - often without the direct ability to get back to anything like the original figures or even an honest accounting of how they arrived at their final figures or, as we have seen with covid vaccination and mortality data, numbers that seem to be fancifully made up from wholecloth (here, here, here and here). Even the Office of The Statistics Regulator has acknowledged that the ONS at times has produced flawed and unreliable data that is unfit for purpose (here and here). As such, we should all be calling for the ONS to produce raw data tables, and not accept data from them that has been modelled using per1000 or ASMR as these are now seen as simply yet another way that the UK ONS are manipulating statistics to make things ‘appear’ or ‘disappear’ as needed. One need only look at the ONS table below, taken from here, and see that the total category percentages of live births (7 + 89 + 3) adds up to 99%, while the total category percentages of still births (65 + 34 + 1) adds up to 100%, to see that even minor mistakes bleed through (as stated above the pre-term percentage is 7.6%, which means 0.4% of babies are spread in some way between term and post-term). Why were they happy to use one decimal place on the left of the table, and no decimal places on the right?

From the text on the ONS’ own report it appears that of the preterm deaths, 50.2% were extremely pre-term deaths, 6% were very pre-term, and 1% were moderately pre-term. The overall average number of deaths across all three strands was 23.5%.
The question becomes - how do we appropriately address the fact that 5.7% of the babies born at CoCH will be extremely pre-term, and that while the protocol would be that in an ideal world they are transferred to Arrow Park or LWH within 6 hours, there will still be some that may die before they are able to be transferred. Similarly, how do we also account for the fact that the extremely underweight category includes babies born between 800 grams and 1kg, who CoCH were permitted to care for under their Level 2 LNU rating at the time? Given that the numbers are so small, I have chosen to leave them in as the nature of how CoCH appeared to operate (see above and in my previous posts) suggests, these poorly neonates were more likely to die at CoCH than anywhere else - and we still don’t know how many were transferred out only to die shortly after arriving at their new destination.
The resulting table comes out to an expected 6 deaths per year (more than double that which was actually occuring prior to 2015, and double that which was forecast by the RPCPH report - which still means the neonatal nurses had been doing 50% better than expectation both prior to 2015 and after 2016), and 9 expected deaths during the 18 month (1.5 year) period, but…
This number still needs some qualifiers.
And it is still only a best case scenario.
(Or a worst case scenario for the poorly neonates)
We have possibly accounted for the variation in Extremely Preterm deaths by leaving them in because, statistically, they were born at CoCH and therefore they had some (and possibly all if they died before transport) of their interactions there. Also, more than 75% would have been between 800 grams and 1000 grams and thus would have stayed anyway. However, we are still missing the number of neonates that would have died in the first days after discharge - possibly adding 2 more deaths per year based on the infant readmission and mortality rate. We are also still missing the number of neonates born and stabilised on the CoCH unit, but transferred out for one reason or another to another facility where they subsequently passed away. This would include the number of deaths in term babies with congenital defects or health conditions that might have seen them transferred to the neonatal unit for short term high acuity care - for example, babies with congenital cardiac or other defects being monitored closely while awaiting transfer to Alder Hay for surgical repair. The CoCH FOI did not disclose the number of deaths in live-born term or post-term babies (38 - 42 weeks gestation), but estimates from other sources range from 3.1 to 3.7 per 1000 live term or post-term births - or between 7 - 8 term babies per year for CoCH.
While we have seen that the neonatal nurses were actually delivering at 50% below expectation in most years, based on these more complicated and hopefully more correct numbers we can now see that during the 18 months from January 2015 to June 2016 the unit may have run at the reverse - an excess death rate possibly as high as 47%, but more realistically at somewhere between 30-40% when those qualifying factors are accounted for.
Using this revised set of numbers and accounting for all of the qualifiers, we could conclude that there are approximately 4-5 excess deaths during the period. Or none, if we factor in the term and post-term deaths.
The question for you to discuss now is:
Are those possible excess deaths sufficiently explained by: (i) the change in higher acuity status (from Level 1 SCBU to Level 2 LNU); and (ii) the staffing shortages that saw neonatal nurses caring for two or more 1:1 neonates at the same time?
Or
Are they explained potentially by the iatrogenic (multiple procedures increases a neonates risk of dying by as much as 50%) and nosocomial (bacterial or viral infection, sepsis and NEC) factors?
Or
Is it possible that there was something nefarious going on?

I want to emphasise here that I believe that with the term and post-term deaths, this means CoCH very likely broke even… i.e. that the potential excess was really a balancing out of the 50% under that midwives and neonatal nurses had been heroically saving during the years pre-2015. The change in acuity, the policies and boundaries being walked all over, and the potential for other issues (like bacterial and viral infection that we see in so many of the subject neonates) all simply acted to make the unit ‘break even’. For the sake of all current and future parents, I hope every hospital can achieve the 50% UNDER expected death rate that CoCH appear to have had prior to 2015.
There’s something in that for all of us.
The next post in our series on the Lucy Letby Trial can be found here.
Someone also pointed out to me today that it can also be to save either the neonate or parents the stress of a transfer, and this too could be a factor. I suppose this may feel like the right thing to do if you can see the neonate may fail to thrive no matter where he or she is sent… but even still, the current trend in the NHS towards not trying to save someone or give them the ability to ‘keep fighting’ is disturbing, to say the least.
the scientific literature is showing that the more preterm, the higher the death rate, AFTER vaccination. The vax schedule has not been studied for preterm, baby weight and mother's milk-feeding (reduces death rate): they are applying it without any consideration to those important variables.
Nurses know this by experience but neonatal docs are like blindfolded!!!
The more developed the baby, the less death rate after vaccination. Based on the data, many pediatricians are suggesting to wait until the immune system is developed (3 years old).
Please read and watch all of this! Your life depends on it, because there's a plan to murder 95% of the global population by 2050… written on the masonic Georgia guide-stones: “Maintain humanity under 500,000,000 … ”
- At least since the 90s, vaccines are weaponized to reduce the population, for example:
1. Adding hCG to infertilize women: lab detected in 30 countries
2. Overpassing the FDA 10 ng limit to human DNA “contamination” by 2000%, thus causing neuro-damage (autism, asperger, tics, dyslexia in 29% of kids, etc.) and childhood cancer epidemic (n.b. leukemia, non-Hodgkin’s lymphomas)
Check soundchoice.org or videos at bottom after this page:
https://scientificprogress.substack.com/p/wake-up-videos
- COVID was designed as a primer for even more lethal COVID haccines:
https://scientificprogress.substack.com/p/the-real-covid-timeline
https://scientificprogress.substack.com/p/not-vaccine-not-gene-therapy-just
https://scientificprogress.substack.com/p/what-do-bioweapons-have-to-do-with
- Wake up videos:
https://scientificprogress.substack.com/p/wake-up-videos
https://scientificprogress.substack.com/p/2050-youll-go-nowhere-and-youll-be
- It's genocide for depopulation:
https://scientificprogress.substack.com/p/depop-vaccines-no-myth
- It’s the masons, who create counterfeited currencies (trillions of dollars and EUROS) and bought the listed corporations, media, healthcare, universities, parties and political careers:
https://scientificprogress.substack.com/p/david-rockefeller-illuminati
Confessions of ex-illuminati Ronald Bernard (all lodges obey the same master, Satan):
http://youtu.be/JAhnCdXqPww
Now, are you really ready for this?:
The full PLAN exposed:
https://scientificprogress.substack.com/p/the-plan-revealed
16 laws we need to exit Prison Planet
https://scientificprogress.substack.com/p/laws-to-exit-planet-prison
Pllllleeeeease, on my knees, don’t believe me, just do your own homework by searching the following in yandex.com, mojeek.com (includes crawl date filter and substack search), gigablast.com, startpage.com, duckduckgo.com (not Google, Bing, Yahoo censors). The key terms to test them? Child Satanic Ritual Abuse, Child Satanic Ritual Murder.
https://www.reddit.com/r/conspiracy/comments/rpn5aj/i_have_found_the_perfect_uncensored_search_engines/
https://www.deepwebsiteslinks.com/uncensored-search-engines-for-anonymous-searching/
If you are a mason or know a mason, ask him to ask his 33° master to put in writing and sign it, who is "the great architect" and that he is not Lucifer. If he refuses, then he’ll know who he is really serving, Satan: tell him to get out of masonry NOW. Sooner or later he’ll be required to trample on a cross to get to a higher degree.
President John Quincy Adams: “Masonry ought forever to be abolished. It is wrong - essentially wrong - a seed of evil, which can never produce any good.”
Confessions of a former mason (Serge Abad-Gallardo):
https://www.ncregister.com/interview/confessions-of-a-former-freemason-officer-converted-to-catholicism
Confessions of ex-illuminati Ronald Bernard (all lodges obey the same master, Satan):
http://youtu.be/JAhnCdXqPww
Confession of 33rd degree master mason - Masons worship deities/demons
https://rumble.com/v294ksc-words-from-33rd-degree-master-mason-rare-video-masons-worship-all-sorts-of-.html
Masonry's Satanic Connection
https://odysee.com/@HiddenTruths:c/Masonry's-Satanic-Connection:4
Masonry's Satanic Doctrine | From Their Own Books
https://rumble.com/v2wg24a-masonrys-satanic-doctrine-from-their-own-books.html
Do Freemasons Worship Lucifer? Evidence They Don't Want You To See
https://odysee.com/@John_4-14:a/Do-Freemasons-Worship-Lucifer%EF%BC%9F-Evidence-They-Don't-Want-You-To-See-%EF%BD%9C-Hidden-Agendas---Walter-Veith:0
Satanic Ritual Abuse and Secret Societies [1995] [VHS]
https://odysee.com/@thisworldworks:1/satanic-ritual-abuse-and-secret-societies-1995:3
Satanic Pedophilia Torture and Blood - Dark Satanic Secrets Revealed
https://odysee.com/@Gmail.com:52/822821884_Satanic-Pedophilia-Torture-and-Blood---Dark-Satanic-Secrets-Revealed:4
UNITED NATIONS LUCIFER AND THE LUCIFER TRUST
https://odysee.com/@dynosarus:c/UNITED-NATIONS-LUCIFER-AND-THE-LUCIFER-TRUST:4
The best way to have a real dialogue about vaccines being weaponized to handicap, infertilize and murder the “over-population” is to start with vaccine contamination: nobody could be in favor of contaminated pharmaceuticals.
1. Carcinogen SV40 in Oral Polio Vaccine: they knew it since the 60s but kept distributing it even until 2016 !!!
2. hCG in vaccines to infertilize women detected since the 90s: still going on
3. Thimerosal, aluminum, Mono-sodium Glutamate (MSG) and other NEUROTOXINS
4. Heavy metals
5. Human DNA 2000% in excess of FDA 10 ng limit (main driver towards brain damage like autism/asperger/ticks, leukemia and non-Hodgkin cancer), probably related to point 7 below.
6. Graphene oxide in Flu and COVID shots but now with anything injectable (even dentist anesthesia, hospital IV, etc.).
7. Carcinogenic SV40 genomic sequences and double-stranded DNA in mRNA COVID shots: the hacked DNA in the cell doesn’t stop producing the poison when the cell dies, but its descent continue the poisoning until the haccinated casualty dies.
8. Bluetooth nano-routers injected with COVID vaccines and inserted with swabs (which explains why they rejected the cheaper non-invasive saliva test).
Proof of criminal intent:
Points 7 and 8
Censoring and blocking 30+ COVID cures
Labeling the most lethal batches with a lethal code (howbad.info)
Blocking the real knowledge of effectiveness v. "adverse event" rate
That proves:
A. There's zero Government control
B. There's zero Manufacturer liability
C. There's zero Media coverage
D. All that, during decades and still going on, not only with vaccines but also with medicines, food&beverage additives, etc. Everything, even institutions have been weaponized!
E. There's zero political action to stop that (except RFK2 in the USA)
A school buddy told me "I know you make sense but if I recognize it's true, I won't be able to enjoy life anymore".
16 laws we need to exit Extermination Planet
https://scientificprogress.substack.com/p/laws-to-exit-planet-prison
If we don’t succeed, they’ll succeed with their 6-sword lethal plan fully exposed here:
https://scientificprogress.substack.com/p/the-plan-revealed
Change goes in hand with the number of awakened! Thank you for sharing this to save lives!
Basic math is not hard. I did realise that your input data was not certain and the math changes the format in which that uncertainly appears. Indeed this kind of output is often presented with great certainly, I’ve seen it in so many of those ‘gold standard’ RCTs. But the message for me was that the same uncertainty with numbers applies to the prosecution case. With small numbers of cases there will be large fluctuations in deaths over a period due to many factors and only contemporaneous investigation and autopsy can decide causes. Thank you for all this fascinating, and distressing, analysis.