


LL Part 12: The Staff Involvement Scorecard
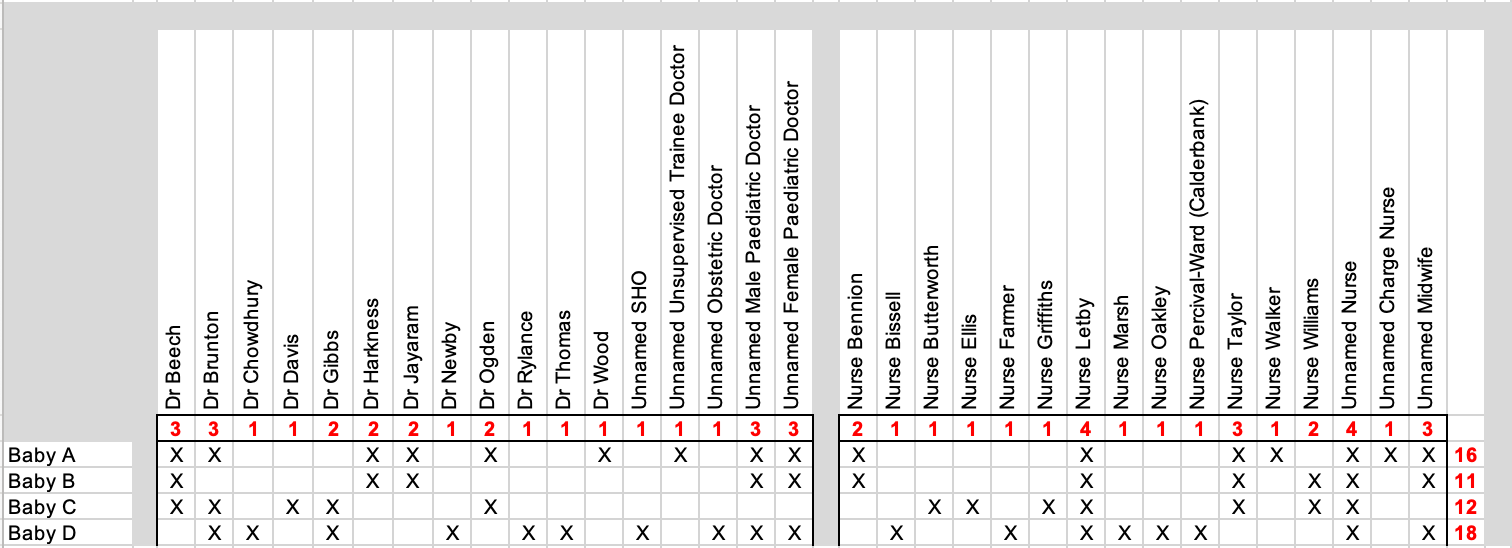
A quick reference scorecard showing the staff involved in caring for each neonate

Following on from the previous article in our Lucy Letby series here.
As you read each of my Lucy Letby case articles presenting the names of and clinical notes detailing care that individual staff (doctors and nurses) provided to each neonate it can if nothing else become a bit confusing. The details are a wealth of seemingly untapped information that you, the reader, could potentially use to be your own hopefully less biased and opinionated ‘Expert1 Witness Wannabe’ (think: Dewi Evans), or alternatively your own less easily led, punishment fixated and self-congratulatory ‘Nancy Drew Defective’ (think: the Cheshire Police).
I have decided to provide readers with an additional visualisation tool to follow along with as you read my ongoing articles on the Lucy Letby case. Each time I deep-dive into the demise of one of the unfortunate and poorly neonates in the case, I will follow that article up with an updated ongoing scorecard showing all the staff that public records show provided some care or were present and either involved in or witnessed the events that unfolded for each neonate. Over time we will build up a quick reference dataset showing both: (i) how many different staff correlate with an individual neonate; and conversely (ii) the number of neonates an individual staff member correlates with.
All joking aside, and unlike the heavily biased scorecard presented to the jury by the prosecution (and to the public by the mainstream media), my scorecard is in no way intended to suggest that any individual nurse or doctor is a murderer. I don’t even want you to be thinking that any other individual is a better ‘fit’ than Lucy. My true aim is to demonstrate to you the absurdity of supposedly seasoned police using an X/Y correlation plot to dwindle down from some much larger number of harm and death incidents (was it 17? 33? 35? or some other number?) and deliberately limited pool of staff members (they left out all the doctors), in order to resolve at either: (a) the person one or two doctors had already put in the frame; or (b) whomever is unlucky enough to be ‘the most correlated’ with ‘the largest remaining cluster of incidents’.
A few caveats before I provide the current running scorecard:
A key limitation of this scorecard is that it has been developed from the clinical and testimonial evidence that was presented in court and has subsequently become publicly available. It does not have visibility of that which is not in the public arena.
We cannot be certain whether the various unnamed doctors and nurses that either (a) gave testimony during the trial; or (b) were mentioned by others who did give testimony during the trial, represent one or more than one doctor or nurse. This is a significant issue both for developing this scorecard AND for our and the jury’s ability to have faith in the consistency and reliability of the prosecution case. As we can see already there are already a large number of ‘unnamed’ hospital staff who come into and out of the case record and correlate with these poorly neonates.
It is a certainty that other doctors and nurses were also directly and peripherally involved in the care of each neonate. With full access to the clinical notes for each baby we would almost certainly identify even more members of staff with involvment. However, there are always instances where one nurse or doctor will assist another with a procedure and the name of that ‘assistant’ never gets recorded anywhere.
Resolution of a scorecard like this (and that which the prosecution showed the jury) cannot provide the viewer with an understanding of the degree to which that person correlates with the patient - were they the designated nurse, the on-call doctor or the consultant with overall responsibility, or were they just someone who was working nearby who got called in as events unfolded? An X/Y correlation plot lacks that additional, yet extremely important, information - and simply makes it easier to say “that person correlates more than these people.”
When we leave aside the fact that parents (and sometimes other family members such as grandparents) have access to these neonates while they are on the ward, the scorecard demonstrates only the minimum number of hands that we can know for certain have touched these poorly babies. It is possible for a poorly neonate to pass through as many as 15 or 20 different sets of clinical hands in as little as 24 or 48 hours. Each staff member is there to perform what is ostensibly a necessary function; whether the purpose is to monitor, examine, perform tests or provide treatment to the patient. Thusly, the interaction of each staff member is usually seen by the others to have been legitimate and each new interaction and report should provide an update to the overall clinical picture for the patient. This ever-changing picture generally, and appropriately, can lead to a change in treatment - a new medication is started or an existing one stopped, or a different treatment or surgery is performed. However, and unfortunately, sometimes egos and powerplay can also see one nurse or doctor overriding the professional decisions of another nurse or doctor and it can sometimes be the patient who suffers. For example, there are several instances in the clinical evidence and testimony of one doctor suspecting sepsis (a systemic infection) in the neonate and prescribing antibiotics, only for another doctor, often one of the junior paediatric doctors on the neonatal unit, to seemingly ignore or override this decision and either fail to administer the antibiotics or to cease the antibiotics that are already being administered. Sometimes the clinical picture may coalesce to make this a correctly updated decision. However, it is doubtful that it was the correct decision for as many of the neonates in the Lucy Letby case as we see it for.
When a patient is harmed either through the omission of an act (not responding to signs and symptoms or failing to provide care that they require), or as the result of an act (providing the wrong care, ceasing necessary care, or care performed with insufficient due skill and attention) and that act or omission results in harm - the term we use to describe this is iatrogenesis.

The result of iatrogenic harm may not be immediately apparent. It may not become apparent even in the same shift, or during the same day. In some cases the iatrogenic cause for and the patient’s resulting negative outcome may never be identified and linked together at all.
The Staff Involvement Scorecard for Babies A-D
The initial Staff Involvement Scorecard listing Babies A to D is provided below:
The next post in our Lucy Letby series can be found here.
Remember that Dewi Evans under cross examination said he did not consider himself to be an expert.
This nails it for me: "The result of iatrogenic harm may not be immediately apparent. It may not become apparent even in the same shift, or during the same day. In some cases the iatrogenic cause for and the patient’s resulting negative outcome may never be identified and linked together at all."
In the absence of direct evidence of harm (correct me if I'm wrong but there was none presented?), why is it presupposed that the indirect harm leading to death (if indeed it was not a natural death) has to occur in the same shift as the death?
It doesn't even require a great deal of thought or logical capacity, does it? Unless, your faculties are subverted by dogma, I guess?
So many questions that should have been asked... But, hey - "found guilty in a court of law"... So...
Here in Scotland I can guarantee you, that the evidence would not have passed the evidential threshold, the fact that the PM’s are not in the evidence chain is disconcerting. As you know inference or hearsay is not evidence, much like the insulin poisoning, with no tangible evidence, which should have been struck.
Until these PM’s are produced we are pissing in the wind, it beggars belief that Goss allowed “expert witnesses” to traduce the PM’s.. not even produced as evidence, both the conduct of Myers and Goss trouble me, as it should all.