


How The Manipulation in Most Covid-19 Studies Works
Cohort Bias: How they make the Pro-Vaccine Covidian Omelette

This morning I happened to listen to the most recent Dark Horse Podcast (number 162) with Bret Weinstein and Heather Heying.

From around 1:22 they discuss a paper by Wanzhu Tu et al called: SARS-CoV-2 Infection, Hospitalisation, and Death in Vaccinated and Infected Individuals by Age Groups in Indiana, 2021-2022.

As I listened to Heather and Bret discuss the egregious and misleading bias used to manipulate some of the findings made with regards to vaccine efficacy - I realised that there have been several flavours of the same cohort and statistical manipulation played on an unsuspecting public (and amplified by the mainstream media) during the last three years. I believe the various basic flavours of this manipulation by cohort biasing needs a simpler explanation…
So for those of you with more advanced understandings of cohort-based clinical trials and statistics, I apologise. Please bear with me as I try and explain this in a way my grandmother or ten year old son might understand.
Fair Cohorts
I want to begin by recognising that there are at least two types of what I will call here: Fair Cohorts. There may be others, but I believe these are the two most basic that we commonly observe.
The Population Matched Cohort
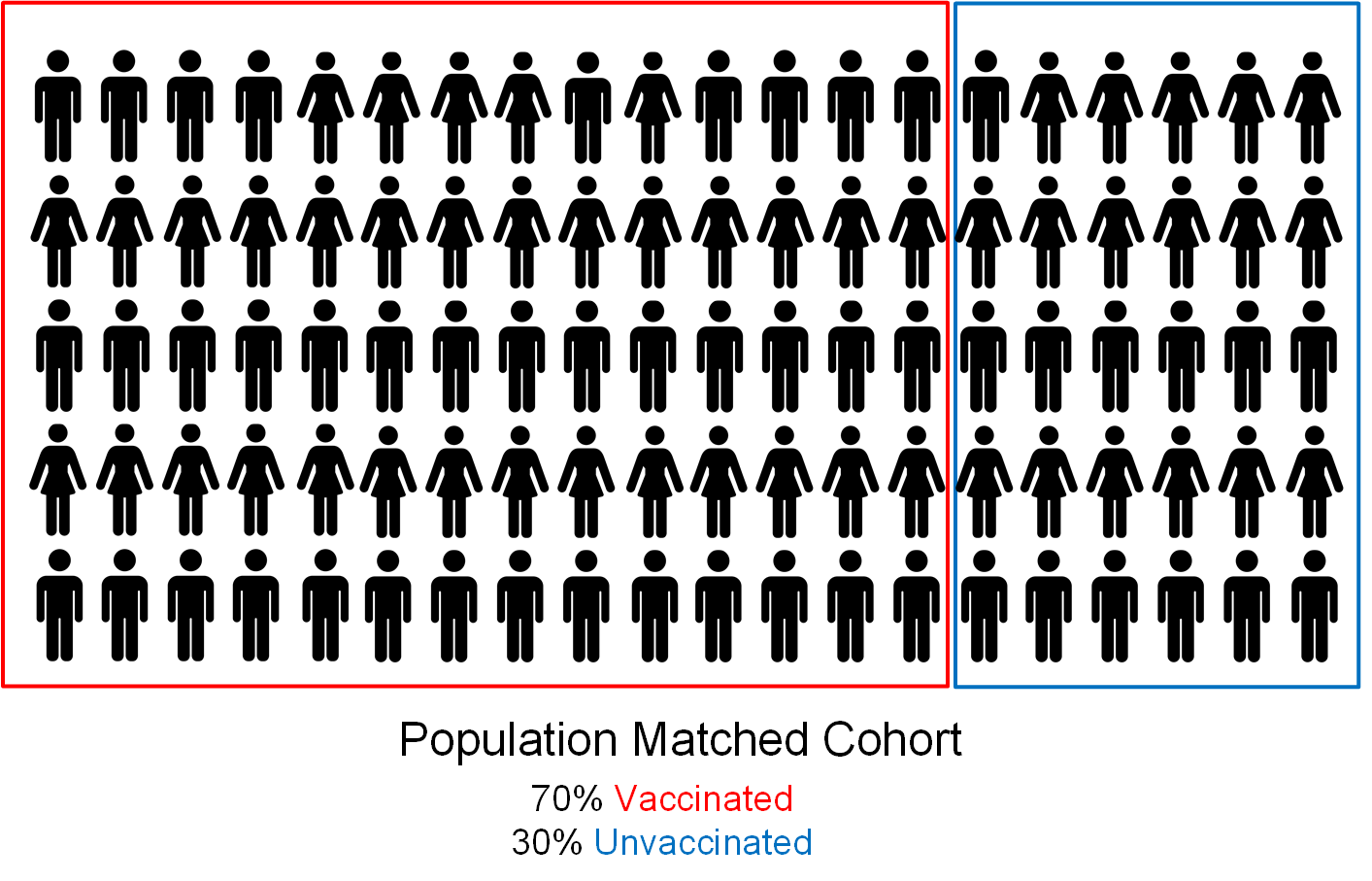
The population matched cohort would prefer a group of randomly selected participants collected from the population at large but with the same percentage weightings of participants with or without the variable under observation (for this post we are doing something common to several widely promoted academic papers: assessing Covid-19 infection severity in two groups: vaccinated and unvaccinated).
Any analysis of the population matched cohort either: (a) corrects resulting output statistics for the known difference in group size; or (b) looks at other aggregate or statistical determinants like overall effect on or change to each group as a result of the outcome of interest (for example: absolute risk reduction or ARR).
The True Matched Cohort

The true matched cohort seeks matching pairs of participants. Participants should be carefully controlled for confounders like age, gender, ethnicity, exposure and so on. It is possible to do a matched cohort study and control for the most important relevant factors and ensure that the potential for bias is minimised, as long as the authors also recognise the potential for any confounders not directly managed in their cohort identification process.
However, one type of matched cohort study, called the matched case-control study, has been seen to deliver variable and sometimes incredible results. The argument often made by authors of case-controlled studies is that it is valid to ignore the matching variables when analysing the matched cohort data (presumably, because they are case-controlled). However, this argument is entirely falacious because it can be very difficult to account for all potential confounders between two such heavily curated groups of individuals. And, as we have already seen (here), some studies do such a terrible job of this fundamental case-control cohort-matching step that they, possibly (or probably) deliberately, produce a heavily biased result that is most likely the outcome sought by the authors or their funders.
Unfair Cohorts
The following cohorts are examples most often seen in the pro-vaccine Covidian literature - that is, the academic papers published by members of the Third group from yesterday’s post. These cohorts are almost always seen to be unfairly weighted in favour of an outcome - almost as though they start with a conclusion they want to prove (for example, that the vaccines are safer or more effective than catching Covid-19 and any natural acquired immunity) and seek to create a science-y sounding explanation for a ‘bent’ cohort that will deliver that result.
The Biased Population Matched Cohort

In this example, members of one group are re-classified as being (or still being) members of the other group. As we can see in the diagram above, 10% of the unvaccinated cohort are actually people who have received the jab, except that they received it recently and within a period that the authors have arbitrarily chosen to treat as though it hasn’t happened yet. This cross-over period has been variously seen as 14, 21 and 30 days depending on the health authority or study authors and the hypothesis they seek to support. For reference: the period after which you have received a medication starts from when the plunger on the needle in your arm is depressed and the medicine is delivered into your muscle or vein… not some arbitrary number of days or weeks after simply because it suits a narrative. One issue this misclassification issue creates (I would argue, intentionally) is that people who have had an immediate or temporally related medical issue following vaccination are treated clinically, and in official statistics and pro-vaccine comparator studies, as unvaccinated. This has allowed even health issues that are clearly caused by the vaccine, like an immediate anaphylactic allergic reaction, to be reimagined as an adverse outcome (or death) caused either by Covid-19 or some allegedly pre-existing condition.
While this misclassification of vaccinated as unvaccinated issue can be identified in many pro-vaccine papers, the UK Office of National Statistics (ONS) mortality data by vaccination status is a very public example of government produced biased population matched cohort data. The vaccination status misclassification issue has been widely reported by one group in the UK - Fenton, Neil, McLachlan, Craig et al - (here, here and described in video and video). As a result of their work, the UK Statistics Regulator has acknowledged the issue and agreed that the ONS data is flawed and any claims made about vaccine effectiveness using the ONS data are unfounded (here and here).
Biased True Matched Cohort
A new approach to biasing matched cohort studies has been to look at vaccinated and unvaccinated people who have a medical record that includes a positive PCR or antigen test for SARS-CoV-2. On first blush this may seem to be a fair evaluator, however, as Bret and Heather discussed in the Dark Horse podcast, that is not really the case.
The biased true matched cohort draws what are often claimed to be matched pairs of people who have medical records that include either vaccination or a positive test result, and evaluates such things as the number of people in each group who attend the emergency department or died with Covid-19 related symptoms. However, the starting premise of such studies is already biased in favour of the vaccine. This is because the starting participant set from which the cohort is selected includes: (i) (almost) everyone who has ever been vaccinated (because their vaccination is recorded and therefore, even for those with no previous medical record, creates a medical record for them); and (ii) only those unvaccinated people who happened to have either been hospitalised with severe covid and had a positive test result as a result of that hospital admission, or those who have considered their symptoms sufficiently serious that they elected to voluntarily go and undertake a health-service administered test. By April 2022 the Institute for Health Metrics and Evaluation (IHME) had reported that at least three quarters (76%) of the US population had been infected with Covid-19 at least once, and that number rises to 85% for the UK population. The issue for the biased true matched cohort is that the cohort identification process completely omits the vast majority of unvaccinated individuals who have had either a very mild infection, or who tested positive at home using one of the at-home antigen tests that work like a pregnancy test and do not need to be sent into a laboratory for processing. Omitting these people from the cohort selection process biases the unvaccinated cohort to being mostly those who had a severe Covid-19 infection - at least severe enough that they approached a health clinic or emergency department for care. The selection process makes it easier to find a person with similar demographics who had mild or no reported Covid-19 symptoms from the much larger pool of vaccinated health records to match your hospitalised unvaccinated person to - thus allowing you to create the unfair impression that the vaccine is safer and more effective than being unvaccinated.
Heavily Biased True Matched Cohort
The heavily biased true matched cohort takes the bias issue one whole step further by incorporating both hospital records bias from the biased true matched cohort and vaccination status misclassification from the biased population matched cohort into the same study - and it is this type of egregious bias laid bare for us in the Wanzhu et al paper.
Wanzhu et al match vaccination and testing data with hospital medical records in order to create a cohort of matched individuals that they claim are: vaccinated people who received at least one dose of vaccine, and unvaccinated people with evidence of previous infection (a positive test result) or clinical diagnosis of infection. The unvaccinated group were biased in two ways. First, they were limited to only that minority subset of unvaccinated individuals who had such a severe infection that it led them to seek treatment in the emergency room. Second, everyone in the study was considered to be unvaccinated up until 30 days after receiving their jab. That’s right… for the purposes of their study, the individual was not counted as vaccinated until 30 days after they received their jab. In this way, any infection they were diagnosed with during that 30 day window was either an infection in the unvaccinated… or not counted as an infection in a vaccinated individual in the results - depending on which of their descriptions you decide to attach significance to. Either they were unvaccinated, or their infection was simply ignored- thus casting the vaccinated group in a more favourable light because a person who has an infection in those first 30 days after vaccination is clearly unlikely to undergo reinfection in the period immediately after 30 days.
Given that the metric given most significance in the ultimate paragraph of the conclusion is that all-cause mortality and emergency department and hospital admissions were both significantly lower in the vaccinated group, evidence of the combination of biases is clear in this work, and the work delivers the exact results the authors set out to prove.
Discussion and Conclusion
When your: (i) unvaccinated cohort consists almost entirely of people with severe infection who either presented to the emergency department (or died); while your (ii) vaccinated cohort that you are matching to contains the entire population of vaccinated people (ranging from those who were never infected all the way to those who died), it becomes very easy to see why even unintentionally your results would be worse for the unvaccinated. And that is being quite generous by suggesting that this cohort bias could have come about unintentionally (which I do not believe to be the case).
It is not enough that the Wanzhu Tu et al study makes one highly significant concession to the unvaccinated - namely that natural immunity provides better protection against reinfection. The remainder of their conclusions all fall in favour of the vaccine - and clearly as a result of their biased cohort selection process. The claim that the vaccines provide considerable protection against (a) severe infection, (b) hospitalisation and (c) death are all biased - tainted by the fact that the unvaccinated cohort would almost certainly have all fallen into at least one of these categories.
The implications of these biases mean that any work that uses these approaches must be carefully scruitinised, dissected, and the effect of the biases taken into account before quoting their results in headlines or further work. I expect this final recommendation is one that the mainstream media, covidians and social media ‘medical influencers’ will continue to ignore.
***
The Law, Health and Technology Substack is a 100% reader supported newsletter. If you like what you have read, please consider becoming a paid subscriber to this work.
***
This is really excellent.
In South Australia 'the authorities' are desperate to keep pushing the 'boosters', as is occurring all around Australia, as there are Covid jab stockpiles to move, and a lucrative mRNA vaccine industry to develop...
Consider for example this article published yesterday on InDaily, with a striking headline:
'Unvaxxed five times more likely to die of COVID: SA research': https://indaily.com.au/news/2023/02/20/unvaxxed-five-times-more-likely-to-die-of-covid-sa-research/
A quote:
"Unvaccinated people are five times more likely to die if they contract COVID-19 than those who are fully-vaccinated, an analysis of South Australian cases has found.
The analysis by the South Australian Health and Medical Research Institute (SAHMRI) found unvaccinated people are also eight times more likely to be hospitalised than those with up-to-date vaccinations."
I'm highly suspicious of this research, and contacted SAHMRI today to seek more info, and received a brief summary. However, I was advised the full report belongs to SA Health and is not SAHMRI's to publish. I've written to the South Australian Health Minister seeking more information.
But it seems to me this is 'research to order' to support the ongoing Covid jab program...