


You Just Can't Make This Stuff Up
The evidence supporting the jabs just gets weaker

Ever since the Covid-19 jabs were rushed along the path from idea to arm, there have been four main groups of people.
First: The people who have been pointing out the issues - first with the harried process, then with the clear lack of efficacy, and later with the unusually high number of side effects and serious adverse reactions. These people get unfairly and inappropriately tainted with terms like ‘conspiracy theorist’ and ‘anti-vaxxer’.
Second: The people who have made small or large platforms for themselves advocating for and supporting the use of vaccines. This group include a large number of GPs, doctors and nurses, along with politicians and journalists and a whole bevy of other ‘visible’ people. Importantly, it also includes the social media ‘medical influencers’ who have, beyond their basic generalist medical training, almost always had no direct qualifications in immunology or virology to support their platform.
Third: Then there are those who have gone miles out of their way to either deny and argue against anything at all raised by the first group, or to create (fabricate) pro-vaccine findings, often cut from wholecloth with poor or no credible scientific method. These people are often referred to as Covidians.
Fourth: The general public, many of whom have been led by the nose by members of the mainstream media, or the second group, parroting the incredible findings of the third group.
The general public (the fourth group) have seen a lot of noise from mainstream and social media types from the second group - either telling them to: (i) ‘get jabbed’; (ii) ‘get your kids jabbed’; or (iii) that something they’ve seen on social media or websites like Substack or Rumble about the jabs is either a conspiracy theory borne of the minds of anti-vaxxers… or just plain false.
Many of my normal readers (thankyou!) know that I have started a series of posts that called Who Fact Checks the Fact Checkers (here, here and here) that deconstructs and analyses the so-called Fact Checks used to discredit people who comment in a way that is seen by the people in the second and third groups as unfavourable towards the jabs. That series of posts will continue to build over the next couple of months - because they are tied to academic research I am doing to investigate and expose the who, what, when and why of fact checking. Some of the early data we have collected shows that many of the ‘fact checkers’ are employed by a small number of organisations with funding from an even smaller number of men who are also, interestingly, tied to the Covid-19 jabs and most of the current globalist narratives (ending private car and property ownership, replacing meat with bugs, 15 minute cities, transgender medical interventions for minors, anti-abortionism, and so on). What is also surprising is that the vast majority of ‘fact checkers’ are young and often only recently qualified… mostly in political journalism and almost never in a domain that would support knowledge of the issues they claim to be critiquing.
Another fact that has also stood out to us is that the so-called ‘fact checkers’ almost never undertake to fact check any of the incredible outputs from the work of the third group - not even when many credible people (sometimes on both sides) have identified that something is wrong with them.
You do have to wonder why…?

Is it perhaps because their financial benefactors (read: funders) only want them looking at issues that impact the narratives they have so carefully constructed and propogated, and profitability of their investments in the jabs?
Perhaps. Or maybe it just isn’t sexy enough to capture eyeballs when you look at the decidedly dodgy science being used by some so-called scientists to support the jabs.
Either way, over the course of the morning I have been following two different threads of discussion on this academic article published on August 11th, 2022 in the (now known to be corrupt - thanks Mr Horton) Lancet. The paper purports to show that Covid-19, presumably rather than the vaccinations, is the cause of increased cardiovascular disease and death.
The Paper

The first thing to note is that this paper is the work of four Chinese and Taiwanese academicians who, whilst all affiliated and working at their home countries, are somehow using a massive dataset from a US company called TriNetX.
The paper repeatedly describes matters in terms of an ‘index event’. However, it is not until the bottom of the final page of content of the paper (just prior to the acknowledgements and references) that we are told the term ‘index event’ is formally linked to administration of the antigen test. The pre-specified trial outcomes were that the individual’s health data demonstrate an ICD-10 code for a cardiovascular event any time from 30 days to 1 year after the antigen test was administered. This, we presume, was to remove anyone from the Covid-positive group who had a cardiac event during or immediately following their infection. However, for a study that seeks to prove that Covid-19 (and not the vaccines) is causing cardiovascular events, it seems odd to exclude people who died or had the onset of cardiovascular symptoms shortly after their test and that would surely be assistive in proving the authors point.
When we review the matched cohort presented on page 6, we see that the covid-19 cohort was not as perfectly matched as the authos would have you believe. The Covid-19 group had consistently higher numbers of people with socioeconomic issues or comorbidities (n=14/16) that have been linked in the academic literature with a propensity for cardiovascular issues directly, or that cause other issues like stress that can lead to cardiovascular issues (see here).
1,665 additional people with housing/economic circumstances problems including homelessness (see here and here)
2,389 additional people with liver disorders including hepatitis (see here, here and here)
2,440 additional people with chronic obstructive pulmonary disease (COPD) (see here and here)
2,776 additional people with diagnosis of depression (see here, here and here)
1,895 additional people with sleep disorders (see here and here)
For example, one recent study looking at homeless people during Covid-19 saw that people who are homeless are 1.6 times more likely to smoke, 4 times more likely to have issues with alcohol consumption, and nearly twice as likely to have atrial fibrillation, diabetes and chronic lung disease.
Instances where the control group had more people with a particular comorbidity than the Covid-19 group were rare (n=2/16), with the maximum swing in the control group’s favour being obesity (n=569). This meant overall that the group of interest, the Covid-19 group, was pre-loaded with individuals with a higher propensity for the cardiovascular diagnoses - which were the events under observation.
The numbers above might not seem to be a large percentage of the overall 690,892 in each group - and we accept that some individuals may have had more than one of the propensity increasing conditions. However, when the differences in frequency of the events under observation (page 7 of the paper) often numbered in the few hundreds (and sometimes in the few tens), this simple and small statistical anomoly takes on much greater significance. The difference in the total number of additional observed cardiovascular events in the Covid-19 group is 4,307 - which could easily be explained by the approximately 14,000 additional predisposing socioeconomic and comorbid factors observed of the population in the Covid-19 group.
Another curious comment comes towards the end of the paper in the form of a claim that therapeutics for Covid-19, such as hydroxychloroquinine and azithromyacin have adverse effects on the cardiac system. This is referenced to another chinese paper which, while acknowledging that hydroxychloroquinine is effective in patients with Covid-19, claims it is cardiotoxic and seemingly more deadly than Covid-19 itself.

What the authors of either the paper we are reviewing or the second paper don’t tell you is that the underlying paper they reference this cardiotoxicity claim to was a review of cardiac and connective tissue issues in mostly female Lupus patients who had been taking hydroxychloroquinine for a median of 7 and maximum of 35 years. No Covid-19 patient would have been taking hydroxychloroquinine for more than a matter of days to weeks, and therefore would never be at risk of the cardiac and connective tissue disorders found in the long term use study. The mention of cardiac issues tied to hydroxychloroquinine was at best misleading, and at worst factitious.

The Data

The methods section of the abstract tells us that the TriNetX dataset includes more that 42 million records from between January 1st, 2019 and March 31st, 2022. For reference, this suggests that the TriNetX dataset incorporates almost 12.7% of the USA population - or around 1 in every 7 US Citizens). The eligibility criteria for the study required that the person have no prior cardiovascular ‘complications’, be unvaccinated, over 20 years of age and not have any neoplasms (abnormal growths that may or may not be malignant) prior to having undergone a Sars-CoV-2 test. They also had to still be alive 30 days after the test. Only a little over 4.1 million (just shy of 10%) met these requirements and were eligible for inclusion. After a process they describe as propensity score matching, two ostensibly identical groups of 690,892 individuals remained - one who is described as having ‘survived Covid-19’ (positive antigen test) and the other who presumably never had it and are therefore labelled as ‘controls’ (negative antigen test).
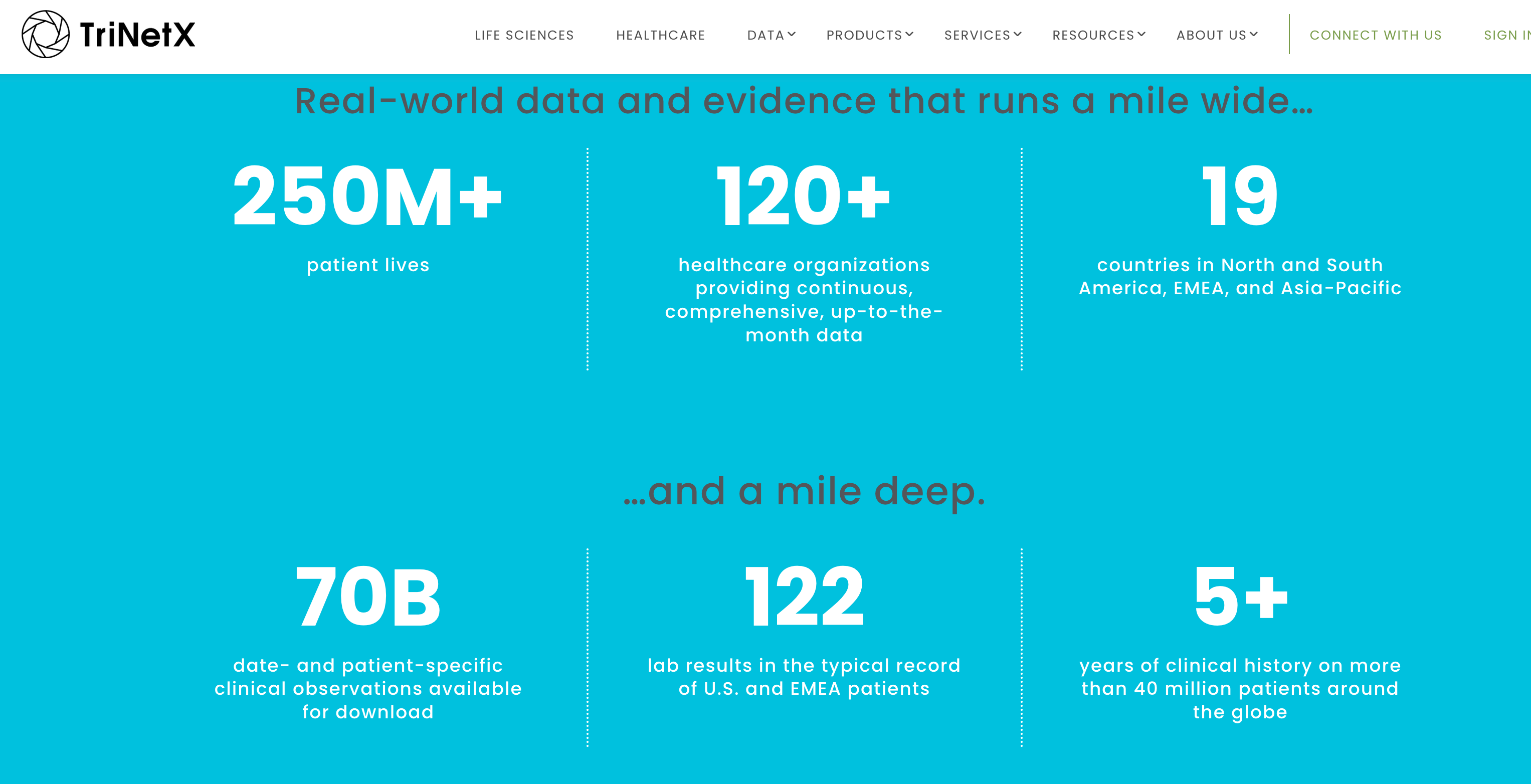
TriNetX are a company that provides aggregate statistical data, usually based around ICD-10 coding. They claim to have access to the EHR of over 250 million ‘patient lives’ (or around 5/7ths of the US population) from 120 different health partners. The description of their data as ‘patient lives’ seems to support the idea that they deal in synthetic data rather than the real-world data they claim on landing at their website - especially when they later go on to describe their dataset as ‘containing 5+ years of data on more than 40 million patients’.
TriNetX are partnered to and work with: (i) Medidata who provide a product they call the Synthetic Control Arm - essentially synthetic (fake) patient data for use as the ‘perfect’ or ‘best-case control’ in comparitor studies; and (ii) Datavant - who only provide synthetic patient data. Both Medidata and Datavant have received funding from and been involved in the awarding of prizes for realistic synthetic patient data from the Bill and Melinda Gates Foundation (BMGF). TriNetX, Medidata, Datavant and Syntegra are all involved in a large consortium to create and deploy realistic synthetic health data that is funded jointly by NIH and BMGF. The question this creates is whether the data used in the study in the paper above was actually real aggregate patient coding data, or synthetic data - given that it comes through an organisation that is so heavily involved in and partnered with organisations that produce synthetic health data. Finally, academic papers partly funded by BMGF outside China actually describe the TriNetX product as a ‘data model’ similar to PCORnet or OMOP, rather than as a patient records dataset.
Several others have also noted that TriNetX deal in synthetic data:
And that more than 60% of the more than 500 Covid-19 ‘trials’ like this one have used Medidata or TriNetX synthetic data:
Other reviewers have commented on the apparent lack of vaccinated individuals in the 42 million strong dataset - especially given that America was boasting more than 80% first dose and 60% second dose uptake at the end of the inclusion period:

Others have called the study dishonest:

TriNetX are also partnered with Pfizer. Make of that what you will…
And the senior author (James Cheng-Chung Wei) has previously worked on research funded by and coauthored with Pfizer employees (here, here and here)

Conclusion
Overall, here we have another paper published that seeks to deviate attention from the cardiac harms actually being caused by the vaccines - through a clearly factitious (made up by humans) claim that Covid-19 causes the increase in cardiovascular disease. The authors of this paper use data from a company that claims to deal in real-world aggregate patient data, yet that company is described by others as providing a data model, and synthetic data. The authors claim to have perfectly matched (their words, not mine) the Covid-19 and Control groups - yet what we find is that individuals with comorbidity that predisposes cardiovascular conditions are found in the Covid-19 group at an increased rate of more than 28 to 1. This biases the Covid-19 group to cardiovascular conditions and the resulting outcome is simply a demonstration of this bias. However, the authors erroneously claim that the over 4000 additional cardiac events seen in the Covid-19 arm are the sole result of the effect of Covid-19 and completely ignore the easily identifiable bias in their conclusions.
This paper is endemic of many published by members of the third (Covidians) group in our introduction in the last 2-3 years that make claims about the Covid-19 condition, and in promotion or support of some other aspect (such as the vaccines). It is an acute example of why more effort must be made to critically appraise such works. Unfortunately those in the second (medical, mainstream and social media ‘medical influencers’) group described in our introduction tend to promote Covidian works like this as truth, and in doing so are actually the ones spreading misinformation and lies.
***
The Law, Health and Technology Newsletter is a 100% reader-funded work. If you like what you see, please consider sponsoring this effort by taking out a paid subscription.
***
TriNetX makes me very nervous. I can see a situation in the near future where main stream medicine only accepts studies that use its black box data, and who knows what's really in that black box. Based on their claims of having all that data available, they must have quasi clandestine contracts with big EHRs such as Epic.
Thanks for an excellent dissecting job. So grateful for people like you. Keeping me sane. ❤️