


Are vaccines life-saving miracle medicines or is there more to the story?
An Open Letter To a Family Member - Part 1

Last night during a conversation we were having you first lauded the CSIRO as one of the most trusted agencies in Australia, and then contradicted that statement by stating that there were issues at the CSIRO surrounding the COVID vaccine and the fact that we would never know the truth. You followed that contradictory statement with... but that’s one vaccine. You can’t categorise them all in one bucket, calling them bad, when there is hundreds of years of science backing them.
When I pointed out that the science backing them in every case also had issues, which is true if for no other reason than because true science should never consider anything settled and should always be open to correction, the response you gave was shaped around one of the more common empty counter-arguments we hear nowadays...
“Why do 0.000004125 percent of the people on earth think they have a better idea of what’s going on than the scientists who have researched vaccines for over one hundred years?”
I could point out that there is nobody on the planet who has been researching anything, let alone vaccines, for over one hundred years for an entirely obvious reason. The average researcher doesn’t start their research career until into their twenties and, ignoring the biblical Methuselah who was claimed to have lived 969 years, only one Frenchwoman named Jeanne Calment who passed away at 122 years of age in 1997 has been verified to have lived over 120 years - making her effective adult life 104 years.
However, and here comes the spoiler alert. While Ms Calment was a shrewd woman who managed to outlive her entire family including her grandson and live the last quarter of her life on a life estate contract for her apartment that eventually paid her more than double what the property was worth, she appears to have never researched vaccines. Okay... so no individual has researched vaccines for over one hundred years.
That was perhaps a little pedantic of me. So, leaving that aside, I could approach the question from a perspective of your intent, rather than your literal words. Let’s consider the claims that there is hundreds of years of science backing vaccines, and that they have been researched for over one hundred years.
Some of my readers know that my twelve-year-old son has had a several-year love affair with the history of Egypt, the language of hieroglyphs, and the research outputs of people like Professor Mummy, Professor Bob Brier. Because of this, the root history of smallpox is something I have become familiar with. You see, my friend, the history of smallpox is inextricably linked to the history of Egypt and her surrounding empires. Smallpox is a disease that is believed to have appeared around 10,000 BC in the agricultural plains of Africa. It was spread to India by Egyptian merchants and there are even examples of smallpox sores found on the faces of pharaonic mummies from the 18th and 20th Egyptian dynasties (1570-1085 BC). Smallpox would go on to become rife in Europe and around the world at a time when people living in the new towns and cities cohabited together with parents, grandparents and sometimes even their animals in small one-room dwellings, sleeping together on rags on the floor with the infected, and not always removing the dead for days after they succumbed to the disease. Smallpox at that time, like many of the other household name diseases we have been taught by propaganda to fear during the last several decades, was predominantly a disease of unsanitary and overcrowded conditions.
While the Plague of Antonine is believed to have been smallpox during the final years of the Roman Empire, and the Spanish and Portuguese conquistadores spread what is believed to be smallpox throughout the middle and south Americas, humans were not, as the sensationalist and pro-vaccine like to claim, at risk of being wiped out by smallpox. Rather, we had lived with it for so long that there were likely more people who had antibodies and natural immunity to it as there were people who might have been susceptible - had they actually been exposed. In fact, and in contradiction to the Jenner story and vaccine myth generally, it was common knowledge even as far back as the 27th Dynasty, when Persia ruled Egypt in 430 BC and right up to the Macedonian Ptolemaic period when Cleopatra and Marc Antony were in power, that the infinitely larger group of people who survived smallpox developed life long and absolute natural immunity to the disease, and that maternal immunisation effects or humoral immune response was passing to the infants of mothers who had this natural immunity both through the placenta and during early breast feeding.

History tells us the first vaccine was developed for smallpox in 1796 - a little over 220 years ago. Perhaps this is what you were actually referring to with your hundreds of years claim. However, while Jenner called his process vaccination (after vacca, for cow - and in spite of the fact that Jenner believed smallpox actually arose from a condition in horses known as grease), the process medically was termed inoculation by variolation.

Variolation with Jenner’s vaccine was extremely unsafe and carried significant risk to the recipient. The original source for Jenner’s first singular vaccination was fluid from sores on the hands of milkmaids believed to be caused by cowpox. With no control for confounders such as the very real possibility of prior exposure and immunity to smallpox, when Jenner variolated an eight-year-old boy with this cowpox fluid and after exposure to smallpox the boy failed to succumb to the disease, he proclaimed his new treatment on the basis of this one poorly controlled experiment created lifelong immunity. Later clinicians would claim ostensibly on the basis of their own research (but more likely motivated by the need to keep the vaccination incomes rolling in) that Jenner’s vaccination only created immunity for three years, or later even, only a single year. These contradictory claims created the first example of an industry for revaccination or, as we term it now, boosters. Jenners experiments also provided the first examples of the now ubiquitous poorly controlled and biased vaccine studies that proclaim absolute efficacy but are equal parts based on cherrypicked data and incredible lies

.In spite of his claim that vaccination with fluid from cowpox sores would provide protection from smallpox, the fluid Jenner went on to use for variolation for many years didn’t actually come from cows or cowpox sores. Rather, he removed it from vesicles of the disease known as grease that were found on the legs of horses. Over the next several decades clinicians would go on to use fluid collected from a variety of similar looking but entirely different diseases that infected many different animals. It was not uncommon even for the fluid in some communities to have been drawn from goat pox. The purulent fluid passed between and used by doctors at the time would become known as vaccine virus - indicating that it was intended to create as much as cure an infection in the patient.
The hope behind the variolation process was that by infecting the person with the disease in ostensibly optimal conditions, that is, when they appeared to be healthy and in the setting of their choosing, they would fare better for the experience and their body would develop the life-long natural immunity the Egyptians and Greeks had identified over one thousand years before. However, things didn’t always go to plan.
The alleged cure Jenner claimed as his own invention was being better done by the Chinese hundreds of years before and, rather than involving pus collected from sores on cows, the Chinese method collected humoral response from sores on infected humans for use as their vaccine medium. Ironically, it appears the Chinese process may have been safer and possibly even more effective. However, and in spite of the fact that smallpox outbreaks and elevated death rates repeatedly followed vaccination campaigns, propaganda of the day that was often written by the doctors whose incomes primarily came from performing these variolations proclaimed vaccination to be the safest and most effective medical intervention for treating smallpox. Perhaps it was the fact that performing these vaccinations had become the single most lucrative branch of surgical practice at the time (Vaughan et al, 1922 at p189) that helped these doctors to overlook the infectious outbreaks, physical harm and death that variolation wrought upon communities.

In communities that received inoculation for smallpox it was found that vaccination increased rates of smallpox death and burials by as much as 27%. In fact, and as the work of Dr Elizabeth Fenn would demonstrate in her investigation chronicled in Pox Americana: The Great Smallpox Epidemic of 1775-82, vaccination for smallpox (variola) was as likely to start an epidemic as stop one, dramatically affected the outcome of the American War of Independence, and may have caused the continental epidemic in North America.

Incredibly, while the pro-vaccine doctors of the day were enjoying their lucrative new income stream they also admitted vaccination could kill, but told us vaccination caused mortality for a mere 2-3% of recipients; many of whom without vaccination might have lived long and fulfilling lives and never encountered the disease. They continued to claim that this vaccine-caused death rate was far smaller than the equally specious 30% of people who contracted smallpox that they claimed would die. Unfortunately, the data collected at the time tells an entirely different and disturbing story. The following chart is taken from page 87 of the exhaustive work of Dr Suzanne Humphries and Roman Bystrianyk in their text Dissolving Illusions.

The grey line reports deaths where vaccination was recorded as causative in the death of the patient. The black line reports deaths from smallpox infection during the same year. Even the least educated of us can clearly see that in most years between 1906 and 1922, smallpox vaccination was involved in more deaths than infection with the disease alone. Notice also that in most cases the peaks in smallpox deaths come during, or more often in the year after, the peaks in vaccine-related deaths. This is possibly further evidence suggestive of the contention that community-wide disease outbreaks followed vaccination programs, which is contrary to what we have always been (mis)led to believe - that vaccination programs were a response to disease outbreaks. This is a theme we see repeated over the last 70 years with other vaccine-targeted diseases.
While it is no wonder that the vast majority of countries, counties and municipalities that had instituted mandatory smallpox vaccination programs during the 1800s repealed those mandates, what is truly incredible was that many in the medical and pro-vaccine movement would go on to proclaim the smallpox vaccine somehow wiped out smallpox. Rather, my friend, the evidence appears to actually show that repealing the mandates and ending the vaccine program itself is what eventually stopped smallpox. The vaccination program appeared to be the last bastion keeping smallpox alive.
The next argument most people tend to make, that knowing you I suspect you would make as well, would be something along the lines of:
“But that was an old style vaccine from one hundred or more years ago. Modern vaccines are far safer and more effective!”
Tell that to the victims of the following modern vaccines that were all eventually withdrawn, but only after they had harmed, maimed or killed numerous recipients:
LYMErix: A vaccine intended to prevent the tick-borne Lyme Disease that was claimed to be 75% effective after only the first dose of a three-dose regimen. After 12 months and 1.4mil doses there were many reports of adverse reactions and vaccine-induced arthritis and Bell’s Palsy - which the manufacturer, SmithKline Beecham (now GlaxoSmithKline), misleadingly claimed were occurring at the same rate as the background unvaccinated population. After losing a 121 person class action lawsuit GSK withdrew LYMErx due to what they disingenuously called poor market performance. LYMErix failed to create any immunity at all in 20% of recipients and post-market monitoring linked the vaccine to long-term and chronic diseases for a percentage of all recipients who became known as vaccine victims. LYMErix was an example of a vaccine rushed to market without adequate testing. Further, the media then, as they do now, denied the established link between the vaccine and adverse events.
1976 H1N1 Swine Flu Vaccine: Around 200 soldiers in basic training at Fort Dix fell ill with H1N1 swine flu in 1976. The CDC reported that at least four soldiers were hospitalised with serious pneumonia and that one died. Public health experts panicked and declared a pandemic was coming that would be worse than the 1918 Spanish flu. President Ford released almost $70mil to rush development and release of a vaccine that was proclaimed ‘ready’ several months later. However, and while no pandemic materialised, over 48mil people were vaccinated with the 1976 H1N1 Swine Flu vaccine. By the end of 1976 there were more than 1098 reports of Guillian-Barre Syndrome (GBS) which national health experts wrote off as an estimated rate of 1-in-100,000 vaccinations, claiming this was not higher than the background incidence (source). After more than 20% of the US population had received the vaccine, the rollout was stopped and the whole matter became known as a sorry debacle and a fiasco that had discredited preventative medicine. While today’s fact checkers like to say there is no evidence (here), the former head of the CDC said in 2009 that the 1976 H1N1 Swine Flu vaccine was recalled after at least 25 people, and as many as 32, had died from vaccine reactions (source). That final number, 32 deaths, is further supported by this academic report (source).
2009 H1N1 Swine Flu Vaccine: In 2009 the CDC rushed to recall 800,000 doses of Sanofi Pasteur’s H1N1 Swine Flu Vaccine intended for administration to children. The headline issue was that the already low potency of the vaccine during manufacture had dropped from 18 to 12 percent (a reduction in effectiveness of one-third). Sanofi Pasteur disingenuously claimed that even though their factories and testers had all failed to identify the issue, that academic investigators at a university serendipitously (unintentionally) found it after it had already been administered to many thousands of children was ‘is a measure of how carefully vaccines are checked’.
SK Bioscience’s SKYCellflu and Sanofi Pasteur’s VaxigripTetra: In 2020 Singapore withdrew both vaccines after they were found to have caused the deaths of at least 59 of the estimated 14.7mil vaccine recipients. Even as the deaths continued Sanofi sought to deny the deaths were linked to their vaccine. The withdrawal went ahead anyway (source).
CSL Fluvax: In 2010 Australia’s Commonwealth Serum Laboratories (CSL) Biotherapies division withdrew their FluVax vaccine after evidence showed children were becoming seriously unwell with fever and convulsions at a rate 900% higher than expected and within 24 hours of receiving the vaccine. Nine out of every thousand children were becoming seriously ill with many requiring hospitalisation after receiving the vaccine (source).
GSK’s Pandemrix and Arapanrix: An increased risk of narcolepsy was identified following vaccination with Pandemrix, a 2009 H1N1 vaccine. VAERS, that much maligned database during covid, was the primary database used to identify cases (source). Interestingly, a study funded by BMGF and others in 2018 sought to reverse the findings by claiming that there was not a rise in narcolepsy cases (source) even though: (i) a PHE study showed narcolepsy in 1 in 55,000 people could be blamed on the vaccine; (ii) a 2017 court ruled Pandemrix caused the narcolepsy of a 7yo boy; and (iii) a 2014 court ruled it caused the narcolepsy of a man called john – with each plaintiff receiving £120,000 compensation (source). A court found GSK had failed to warn recipients of Pandemrix’s issues that had been identified to the board in internal safety reports (source). In all, a BMJ study showed Pandemrix caused 72 serious adverse events per million doses, 700% more than a similar vaccine (GSK’s Arepanrix) (source). GSK requested withdrawal of Arepanrix in late 2010 and Pandemrix has not been available since 2015 (source).
Roche Tamiflu: While considered an antiviral, in some countries (like Australia) Tamiflu was administered to young children as a vaccine (prophylaxis). Roche withheld vital information about Tamiflu for more than 5 years, including the fact that Tamiflu had little or no impact on the known complications of influenza infection, such as pneumonia (source). One study saw 119 deaths after administration of Tamiflu (source), while others report that the vaccine caused neuropsychiatric disturbances in adolescents and resulted in at least 50, and as many as 71, deaths (source and source). Investigations also looked into deaths of babies and infants that were laid before the Tamiflu injections and oral suspension (source).
But, I might also hear you say, vaccines never cause the disease, or deaths from the disease, that they are intended to prevent. Sadly there are many examples of vaccine induced infection. For example:
Cutter Poliomyelitis Vaccine: Described as a medical tragedy and in spite of a scientist at a government laboratory issuing a warning that the vaccine had given polio to a previously healthy lab monkey, an estimated 120,000 children received the 1955 Cutter Polio vaccine with 1 in 3 (40,000) suffering abortive or vaccine-induced polio as a result. Fifty-one children were permanently paralysed with polio and 5 died before the vaccine could be recalled (source).
Pfizer-Vax Measles-K: Pfizer-Vax Measles–K, Pfizer’s inactivated measles vaccine from 1960 was administered in a series of three vaccines at one month intervals because, they claimed, it was much less reactive than other vaccines. However, it was found that the vaccine offered limited effectiveness against the disease. In fact, the majority of children who received the vaccine had no detectable levels of measles antibodies when tested one year after vaccination. By 1965 doctors were reporting a new and abnormal measles-like illness they called atypical or vaccine-induced measles that was arising in children in children previously vaccinated with Pfizer’s Measles-K vaccine upon exposure to wild measles. Symptoms of this new atypical measles included rash, swelling, fever, pneumonia, and pleural effusion. Measles-K vaccine was withdrawn by the regulator from the market in 1968 (source, source and source). There were several papers written in the 1970s and 80s that describe ongoing and even elevated rates of related atypical (vaccine-induced) measles infections and deaths in children (here, here and here).
Pertussis (Whooping Cough) mortality had almost completely declined in England and Wales by the mid-1950s when the Whooping Cough vaccine was adopted for widespread use:

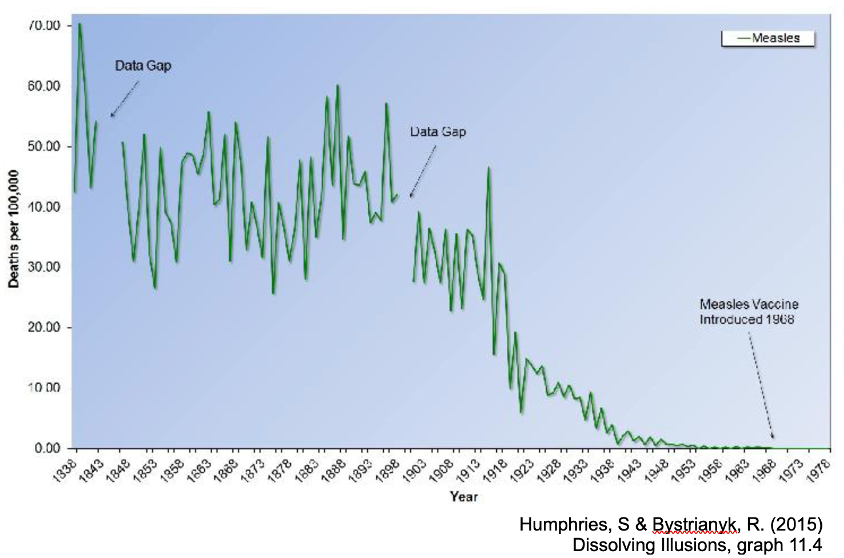
Measles had almost entirely been eradicated in England and Wales before 1968 when the measles vaccine was introduced:
And diphtheria infections in Leicester, England actually spiked dramatically after a large proportion of the population had been vaccinated:

Honestly, my friend, I could go on for days with examples, including the fact that vaccines were the direct cause of a dramatic resurgence in pertussis (whooping cough) infection. I could even demonstrate to you something I think from our discussions you are already aware of: that Covid outbreaks actually followed rather than preceded the mRNA Covid-19 vaccination programs in Australia and New Zealand. However, I believe I raised enough examples to at least show the answer to the question of whether today’s vaccines are safer or more effective than Jenner’s 220-year-old vaccination simply by virtue of their modernity is complicated.
I will end Part 1 of this open letter here. There is more... a lot more. But I think it best if I break it down into separate issues and bite-size chunks.
You are entitled to your beliefs. But, and at the very least, those beliefs should be informed by more than the sound bites we heard growing up. They should be informed by more than the one-sided propaganda that we currently teach doctors, nurses and teachers about vaccines at university. And they should be informed by more than the anti-science claims of people on TV in white coats like Anthony Fauci.
The best advice: If you want to stay healthy, stay away from the medical profession.
https://www.bmj.com/content/387/bmj.q2852 Paediatric RSV 'vaccine' trial 'paused' after X5 infections.
Should be classed as parental neglect to offer your kids for a mRNA trial.